Background
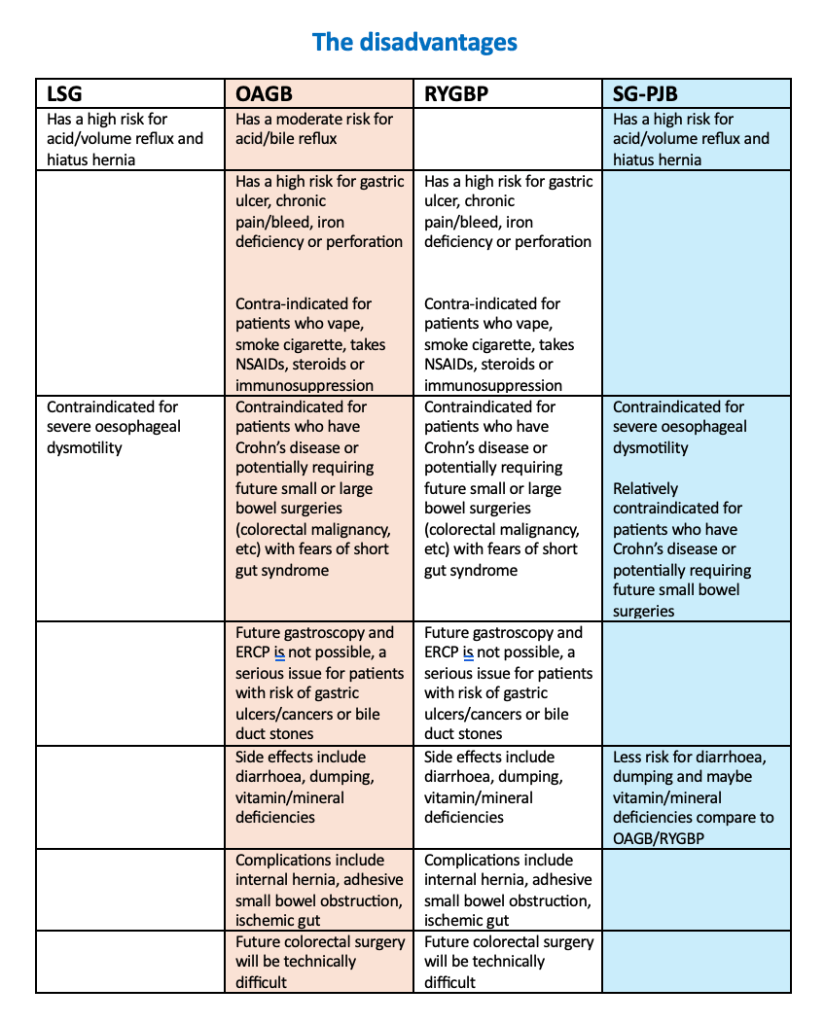
The SG-JB was first described in 2002 by Alamo, a surgeon in Chile to be an effective weight loss operation, to avoid some of the complications of the gastric bypass (mainly anaemia, marginal ulcers, dumping syndrome, nutritional deficiencies, internal hernia) and also to avoid the more aggressive malabsorptive procedures (such as BPD-DS, SADI-S, etc)
- This surgery was first performed around 2004
- Initially the surgery was done with a gastric anastomosis, known as Vertical Isolated Gastroplasty with Gastro-Enteral Bypass in 2006
The surgery was modified in 2012 and became the sleeve gastrectomy with jejunal bypass:
- The sleeve gastrectomy was created using a 36Fr bougie
- The jejunum was divided 30cm distal to the ligament of Treitz
- The small bowel anastomosis was created 250-300cm distal to the jejunal division
- There should be at least 300cm of common channel
Clinical effectiveness
It was found that exclusion of the proximal jejunum (with or without duodenal exclusion) improves weight loss and T2DM control because of incretin (GLP-1, PYY) release from the L cells
- The SG-JB was more effective than sleeve gastrectomy by changing the small bowel anatomy and adding a malabsorptive component
- Studies reported that SG-JB has similar T2DM remission results and other metabolic improvements similar to the RYGBP
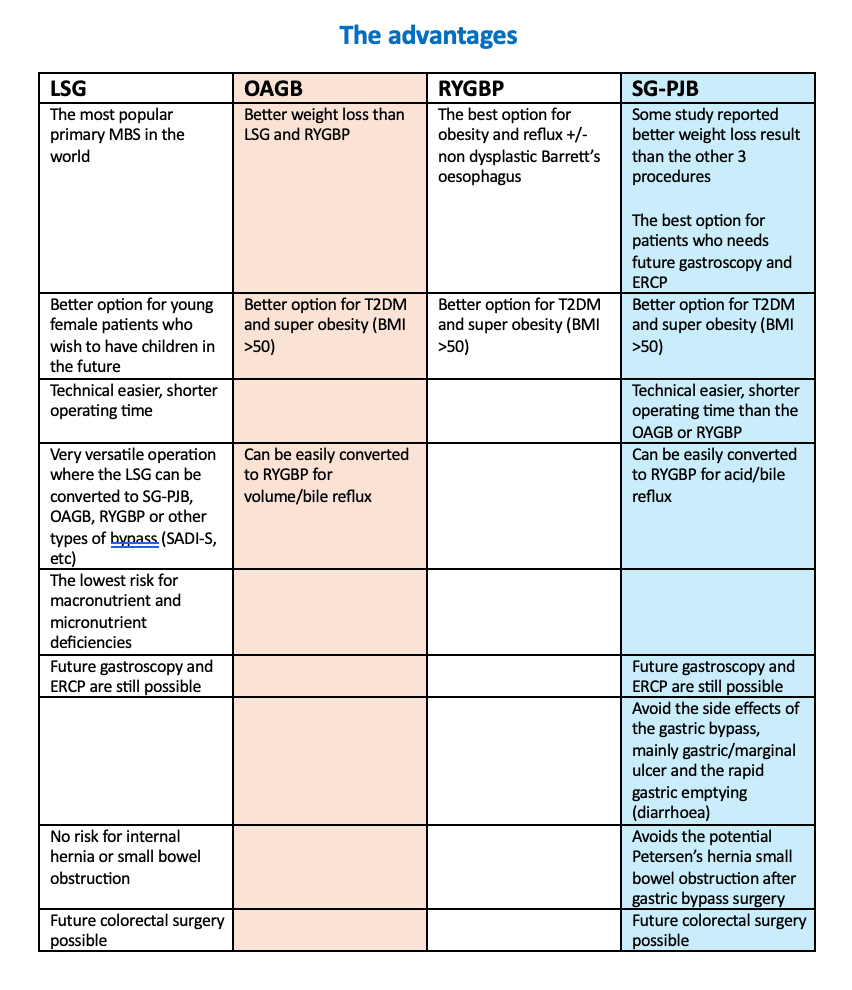
- One study reported that SG-JB is superior to RYGBP in terms of weight loss and less complications
A systemic review and meta-analysis published in 2021 reported that the sleeve plus procedures have better weight loss results than RYGBP with fewer complications
- This has become a common procedure in Asian counties because it is technically easier than the RYGBP with less complications, preserving the pylorus and a longer common channel with less risk of dumping, SIBO and malnutrition
Alamo and colleagues found that with 20 years follow up, there were no alteration in liver function, albumin levels, liver failure, enteropathy or other severe micronutrient deficiency
- Further studies didn’t find any evidence of small intestine bacterial overgrowth (SIBO) or blind loop syndrome, the more proximal jejunum has less bacteria colonization
- This operation is different to the jejunal ileal bypass (JIB), first described in the 1960s which had a lot of enteropathy, SIBO (Bacteroides), endotoxin hepatoxicity, protein-calorie malnutrition and altered bile salt metabolism
One group similarly described a less aggressive 200cm bypass, the sleeve gastrectomy jejunal jejunal bypass (SG-JJB), which may be more appropriate for patients with a shorter small bowel length especially for non Caucasian cultures
In short the SG-JB is:
- A combination of restriction plus hormonal effects with good weight loss results and glycaemic control
- Feasible, safe, effective, reproducible, versatile (can be converted to RYGBP), reversible (of the small bowel anatomy)
- The stomach remnant and duodenum is not excluded, allows future surveillance gastroscopy and ERCP
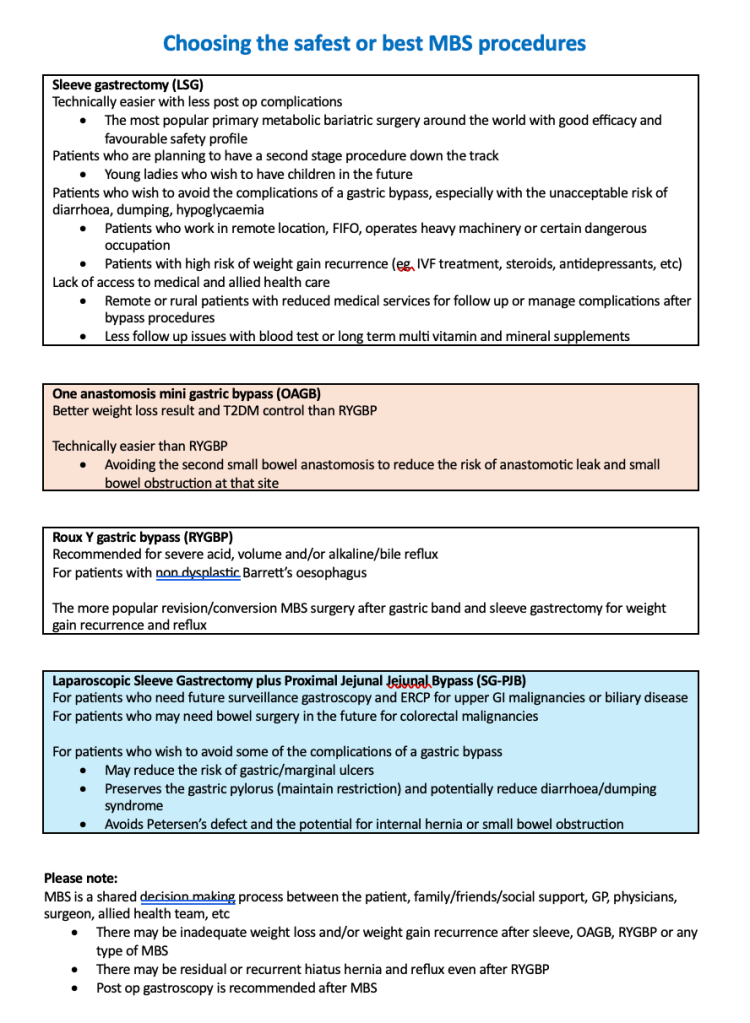
| Options for Laparoscopic Metabolic Bariatric Surgery (MBS) 2026 Patient choices There are 3 common types of primary procedures available: Laparoscopic Sleeve Gastrectomy (LSG) Laparoscopic One Anastomosis Gastric Bypass (Mini bypass) (OAGB) Laparoscopic Roux Y Gastric Bypass (RYGBP) These can be primary or revision/conversion procedures available: Laparoscopic One Anastomosis Gastric Bypass (Mini bypass) (OAGB) Laparoscopic Roux Y Gastric Bypass (RYGBP) Laparoscopic Sleeve Gastrectomy plus Proximal Jejunal Bypass (SG-PJB) Laparoscopic Re-Sleeve Gastrectomy (rLSG) Newer surgery Laparoscopic Sleeve Gastrectomy plus Proximal Jejunal Jejunal Bypass (SG-PJB) *Potentially better weight loss result *Potentially less side effects and complications than a gastric bypass *Easier and a possible alternative to SADI-S and duodenal switch procedures |
References:
Alamo M, Sepulveda C, Zapata L. Vertical isolated gastroplasty with gastro-enteral bypass: preliminary results. Obes Surg 2006; 16: 353-8
De Menezes JE, Azaro E, Mello CA, et al. Analysis of the vertical isolated gastroplasty: a new bariatric operation. Obes Surg 2006; 16: 1261-3
Alamo M, Sepulveda M. The Sleeve Gastrectomy with Jejunal Bypass (Original technique). Journal of Laparoendoscopic and advanced surgical technique 2024; 34 (1): 77-81
Huang CK, Mahendra R, Hsin MC, et al. Novel metabolic surgery: first Asia series and short term results of laparoscopic proximal jejunal bypass with sleeve gastrectomy. Ann Laparosc Endosc Surg 2016; 1: 37-42
Chen G, Zhang G, Oeng BQ, et al. Roux-en-Y gastric bypass versus sleeve gastrectomy plus procedures for treatment of morbid obesity: Systematic review and meta-analysis. Obe Surg 2021; 31: 3303-11
Lin S, Li C, Liang H. Three year outcomes of sleeve gastrectomy plus jejunojejunal bypass: a retrospective case-matched study with sleeve gastrectomy and gastric bypass in Chinese patients with BMI >35 kg/m2. Obes Surg 2121; 31: 3525-30
