This blog provides free general information for anyone who is seeking to understand the newly revised criteria for bariatric and metabolic surgery, not intended as a medical consult. Please seek proper medical advice for individual assessment and management.
Introduction
Obesity is now recognized as a chronic disease with associated chronic low grade inflammatory state and immune dysfunction, which leads to abnormal cytokine production, adipokines, hormones and acute phase reactants and consequently metabolic disorders and associated complications.
For weight loss, resolution of medical co-morbidities/complications bariatric and reduction in mortality, bariatric/metabolic surgery has proven durability, efficacy, safety and cost effectiveness.
Previous criteria for bariatric surgery was published by NIH in 1991. Over the last 30 years we have witnessed an epidemic of obesity and T2DM as well as an explosion in bariatric surgeries performed worldwide. Studies with long term follow up data have successfully confirmed that bariatric/metabolic surgery produces:
- superior weight loss results compare to non operative methods
- significant improvement of metabolic disease and quality of life
- decrease in overall mortality
- safety with a low peri-operative mortality 0.03-0.2%.
Long term studies (over 5 to 20 years) have confirmed the safety, efficacy, durability and cost effectiveness of bariatric and metabolic surgery.
| New criteria This led to a change in criteria for surgery in 2022, published by IFSO and ASMBS. Below is the summary from the recent 2022 ASMBS and IFSO publication regarding the indications for metabolic and bariatric surgery. Metabolic and Bariatric Surgery is now recommended for Caucasian patients with: *BMI >35 with or without medical co-morbidities (Class 2 obesity) *BMI > 30 with metabolic disease (Class 1 obesity) *BMI >30 for patients who did not achieve substantial or durable weight loss or co-morbidity improvement with non surgical methods *BMI >27.5 in Asian populations |
| Class 1 obesity Metabolic and bariatric surgery is recommended for patients with a BMI>30 who has Type 2 DM. Metabolic and bariatric surgery can be considered a treatment option for Class 1 obesity (BMI 30-34.9) who does not achieve substantial or durable weight loss or improvements in comorbiditiy from non surgical methods. Delegates of the 2nd Diabetes Surgery Summit published a position statement in 2016 in support of metabolic and bariatric surgery for patients with BMI <35 and T2DM. Since then many other studies and trials have consistently demonstrated significant weight loss at 5 years with improvement in T2DM, HPT and dyslipidaemia. One trial has been demonstrated that surgery for Class 1 obesity patients to be superior than lifestyle modification for remission of T2DM 3 years after. |
| Class 2 obesity Multiple scientific data and publications have established the safety, efficacy and cost effectiveness of metabolic and bariatric surgery, improve survival and quality of life for Class 2 obesity patients. For patients with BMI>35, current non surgical treatment options are ineffective in achieving substantial or sustainable weight loss plus resolution of obesity related co-morbidities. |
Other indications for surgery may include the ones listed below.
Asian population
It is recognized that Asian patients with a BMI >30 with visceral/central obesity plus metabolic/cardiovascular disease have higher health risk than Caucasian patients with BMI >40 with gynaecoid/peripheral obesity without metabolic/cardiovascular disease.
In Asian populations the prevalence of T2DM and cardiovascular disease is higher than non Asian population in the lower BMI range, hence surgery can be recommended for Asians with BMI >27.5
Extremes of age
Surgery has been performed for patients over 70 years of age with weight loss benefits and remission of co-morbidities but this group has higher post op complications. Surgery should not be performed for those with severe physical/cognitive impairments or end organ damage.
Adolescents <18 years having gastric bypass has proven weight loss results and improvement in cardio vascular co-morbidities. Surgery has been recommended for Class 2 obesity patients (BMI >120% in the 95th percentile) and Class 3 obesity patients (BMI >140% in the 95th percentile).
High risk patients
Patients with a BMI>60 are considered to be especially high risk, with more technical challenges, longer operative time, perhaps ICU/HDU admission, peri-operative morbidity and longer hospital stay.
Patients with compensated liver cirrhosis have an increased peri-operative mortality but the risk is small and there are still significant benefits from surgery (bariatric and metabolic surgery is associated with 88% risk reduction of progression NASH to liver cirrhosis). However caution against operating on patients with portal hypertension.
Bariatric and metabolic surgery has been performed in patients with heart failure as a bridge to heart transplant or left ventricular assist device. There has been improvement in left ventricular ejection fraction, functional capacity and eligibility to receive a heart transplant.
Bridge to other treatment
Bariatric surgery can be performed before other procedures such joint surgery, abdominal wall hernia repair and organ transplant (kidney, liver, heart).
Bariatric and metabolic surgery before hip and knee replacements have been shown to decrease orthopaedic operative time, hospital length of stay and early post op complications.
Surgery before elective abdominal wall hernia repair helps to reduce the risk for impaired wound healing, local and systemic infections and other general surgery post op complications.
Class 3 obesity is a relative contraindication for solid organ transplant and obesity poses technical challenges in transplant surgery. After bariatric/metabolic surgery some patients achieve significant weight loss and improve their eligibility to organ transplant.
Long term results for weight loss and metabolic surgery
Studies of patients who had bariatric and metabolic surgery has a significantly lower risk of new onset heart failure, AMI and stroke compared to matched controls. The long term reductions in cardiovascular risk are particularly obvious in those with T2DM. Some studies have shown that microvascular complications of T2DM are decreased after surgery with 20 years follow up as well as markers for diabetic nephropathy.
Greater weight loss and improvement in T2DM, HPT and dyslipidaemia has been demonstrated beyond 10years after metabolic surgery compared with non surgical controls. Sustained weight loss of at least 15% have a significant metabolic improvements.
Randomized controlled trials has demonstrated that the sleeve and Roux Y gastric bypass was superior to medical therapy ion the long term treatment of T2DM. The STAMPEDE trail is the most well known trial.
Reduction in hospitalization rate for cardio-vascular complications
Metabolic and bariatric surgery is associated with lower risk for hospitalization for cardio-vascular disease in patients with non alcoholic fatty liver disease or metabolic dysfunction associated steatotic liver disease (MASLD), with lower in hospital mortality, acute kidney injury, mechanical ventilation and shorter hospital stay.
MASLD has increased insulin resistance, pro-inflammatory mediators and dyslipidaemia which promotes atherosclerosis and oxidative stress, with increased cardio-vascular risk.
Metabolic and bariatric surgery has been reported to reduce the risk of acute myocardial infarction (by 39%), coronary artery disease (by 37%), haemorrhagic stroke (by 52%) and heart failure (by over 60%). It has been shown to reduce other events such as TIA, secondary stroke, arterial thrombosis and embolism) by 50%.
Reduction in cancer risk
Several studies have shown that surgery reduces obesity related cancers (in particular GIT, hepato-biliary, genito-urinary and gynaecological cancers) and the risk of developing all types of cancers by 11-50% in patients with Class 2 and 3 obesity.
Bariatric and metabolic surgery may also significantly reduce overall cancer mortality compared with non operated obese control patients.
Reduction in mortality
Many studies have demonstrated that bariatric and metabolic surgery consistently report improved survival benefits and lower mortality rate.
The most well known is the Swedish Obese Subject Study (SOSS) demonstrated an adjusted decreased overall mortality by 30.7% in the surgical group compared to non surgical control, with their 2010 patients after 10 years.
Other studies reported reduction in all cause mortality was lower at 5-110 years after surgery, 40% decrease in mortality with a mean of 7 years follow up and life expectancy increased by 6.1 years in the surgical group compared to the non-operated controls.
Revisional surgery
Obesity is now recognised as a chronic, relapsing and multifactorial disease. With the rise in primary procedures there is also a rise in the need for revisional surgery for weight regain, insufficient weight loss, insufficient improvement in medical co-morbidities and surgical complications (such as reflux).
The complexity of revisional bariatric and metabolic surgery is higher than primary surgery with an increased length of stay and higher rates of complications. Hence patient selection is important.
| IFSO Delphi consensus 2023 (Level 5 evidence) The prevalence of obesity (BMI >30) is predicted to rise from 14% (in 2020) to 24% (by 2035) 2 billion adults and adolescents/children will be obese *There is a rapid rise in childhood and adolescent obesity *There is a rise in obesity related co-morbidities and complications (T2DM, cardio-vascular disease, OSA), increase cancer risk, reduced QOL and increase mortality rate But the mechanisms of action are complex, multifactorial and often incompletely understood *The response to metabolic and bariatric surgery is variable, does not necessarily reflect the surgeon’s skill/technique, types of bariatric procedure, patient non compliance or bad eating behaviour Thus the recommendations from the Delphi consensus: *Avoid the use of terms such as restriction, hypoabsorption or malabsorption operations *Use the term “suboptimal weight loss” or “suboptimal clinical response” rather than “inadequate weight loss” or “non response” *Suboptimal clinical response is <20% total body weight loss (TBWL) or inadequate improvement in obesity complication *Recurrent weight loss is >30% TBWL or worsening of an obesity complication From the Delphi consensus 2023 *Sleeve gastrectomy is the common procedure and most suitable procedure performed worldwide but less suitable for patients with T2DM, GOR and NASH *OAGB and RYGBP are more suitable for obesity + T2DM *OAGB with BP limb >200cm increases the risk of protein deficiency *BPD-DS and SADI-S require life long surveillance and nutritional supplements |
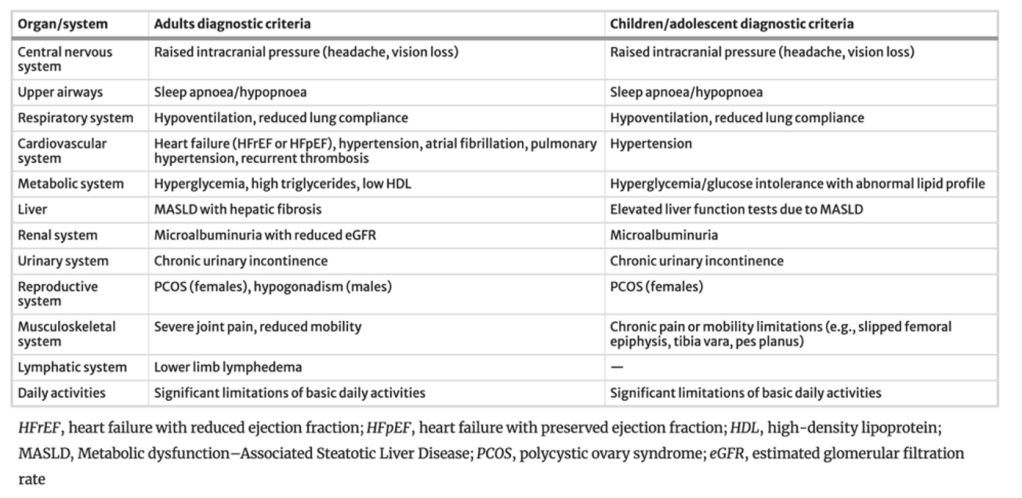
| The Lancet 2025 new definition Recently five metabolic and bariatric surgeons who served as experts to the Lancet Commission on Obesity published a new definition for patients with clinical and pre-clinical obesity *to help identify obesity as a chronic disease, assist diagnosis, stratify risk *to set up a framework to support personalized care, better treatment selection and aligned with chronic disease management standard *enhance surgical candidate selection, reshape perception on metabolic bariatric surgery and increase patient access to medical intervention or surgery Clinical obesity is excess obesity with at least one obesity induced organ dysfunction, eg. pulmonary restriction, liver fibrosis, cardiometabolic compromise *Diagnostic criteria of clinical obesity include specific obesity induced organ impairment, there are 18 criteria for adults (13 criteria for children/adolescents) *Clinical obesity is a disease and require evidence based intervention, which is pharmacological +/- surgical modalities complemented (but not substituted) by lifestyle interventions Pre-clinical obesity is excess adiposity in the absence of demonstrable organ dysfunction *This represents a condition of elevated risk for progression to clinical obesity or associated disease such as T2DM, cancer, mental health disorder *Pre-clinical obesity require risk reductio strategy (lifestyle intervention, medications or surgery) proportional to the level of risk The diagnosis of excess adiposity can’t be determined by weight or BMI alone, which doesn’t describe organ dysfunction, health or illness of the individual or their functional status *Excess adiposity takes into account BMI, waist circumference (88cm for women, 102cm for men), waist to height circumference (>0.85 for women, >0.9 for men), waist height ratio (>0.5), direct body fat measures (with DEXA, MRI) *Excess adiposity is assumed in patients with BMI over 40 Risk assessment takes into account visceral vs peripheral fat distribution, BMI, medical conditions (T2DM, mental health disorder, etc), family history, need for other care (joint replacement, cancer, transplant, etc) Weight loss serve as a proxy for reduced health risk in individuals with pre-clinical obesity Similarly for patients with clinical obesity, weight loss result alone is not a measure of therapeutic success, treatment efficacy should be measured by resolution or improvement of the functional impairments (a collaborative care model) Metabolic bariatric surgery historically has been the only effective anti-obesity treatment, regarded as the gold standard (especially for the RYGBP) although nowadays this term is no longer used *Recently obesity management medications have filled in the gap, shifting metabolic bariatric surgery for the more complex or higher risk patients *Nowadays metabolic bariatric surgery must be seen as a therapeutic not preventative intervention *Nowadays high risk metabolic bariatric surgery may even be seen as appropriate for pre-clinical cases such as optimization for orthopaedic or transplant surgery Viewing obesity as a disease spectrum supports more precise diagnosis and targeted treatment Positioning OMM and MBS as therapy for clinical obesity elevates its legitimacy, improve patient access and integrate into a chronic disease model |
The diagnostic criteria for clinical obesity by organ system in adults and children/adolescents
Bibliography
Surg Obes Relat Dis 2016; 12 (1): 1144-62. Rubino F, Nathan D, Eckel R, et al. Delegates of the 2nd Diabetes Surgery Summit. Metabolic surgery in the treatment algorithm for type 2 diabetes: a joint statement by international diabetes organizations.
Surg Obes Relat Dis 2018; 14 (8): 1071–87. Aminian A, Chang J, Brethauer S, et al. American Society for Metabolic and Bariatric Surgery Clinical Issues Committee. ASMBS updated position statement on bariatric surgery in class 1 obesity (BMI 30-35).
Diabetes Care 2016; 39(9):1510-8. Ikramuddin S, Komer J, Lee W, et al. Durability of addition of Roux Y gastric bypass to lifestyle intervention and medical management in achieving primary treatment goals for uncontrolled type 2 diabetes in mild to moderate obesity: a randomized control trial.
N Engl J Med 2017;376 (7): 641–51. Schauer P, Bhatt D, Kirwan J, et al. Stampede Investigators. Bariatric Surgery versus intensive medical therapy for diabetes – 5 year outcomes.
JAMA Surg 2015;150(10):931-40. Courcoulas A, Belle S, Neiberg R, et al. Three year outcomes of bariatric surgery vs lifestyle intervention for type 2 diabetes mellitus treatment: a randomized clinical trial.
Lancet 2015;386(9997):964-73. Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric-metabolic surgery versus convetional medical treatment in obese patients with type 2 diabetes:5 year follow up of an open-label, single centre randomized controlled trial.
J Am Coll Cardiol 2022;79(15): 1429-37. Mentias A, Aminian A, Youssef D, et al. Long term cardiovascular outcomes after bariatric surgery in the Medicare population.
Surg Obes Relat Dis 2022;18(4):475-83. Ke Z, Zhou X, Sun F, et al. Effect of bariatric surgery versus medical therapy on long term cardiovascular risk in low BMI Chinese patients with type 2 diabetes: a propensity score matched analysis
N Engl J Med 2007;357(8):741-52. Sjostrom L, Narbro K, Sjostrom C, et al. Effects of bariatric surgery on mortality in Swedish obese subjects.
N Engl J Med 2007;357(8):753-61. Adams T, Gress R, Smith S, et al. Long term mortality after gastric bypass surgery.
Lancet 2021;397(10287):1830-41. Syn N, Cummings D, Wang L, et al. Association of metabolic-bariatric surgery with long term survival in adults with and without diabetes: a one stage meta-analysis of matched cohort and prospective controlled studies with 174772 participants.
