Calculations
Total body weight loss (TBWL) is the pre-op weight minus the post op body weight.
% TBWL is the fraction of body weight expressed in percentage term.
Percentage of excess weight loss (%EWL), is calculated using an ideal body weight of BMI 25 kg/m2.
% BMIL is the percentage of BMI loss
% EBMIL is the percentage of excess BMI loss

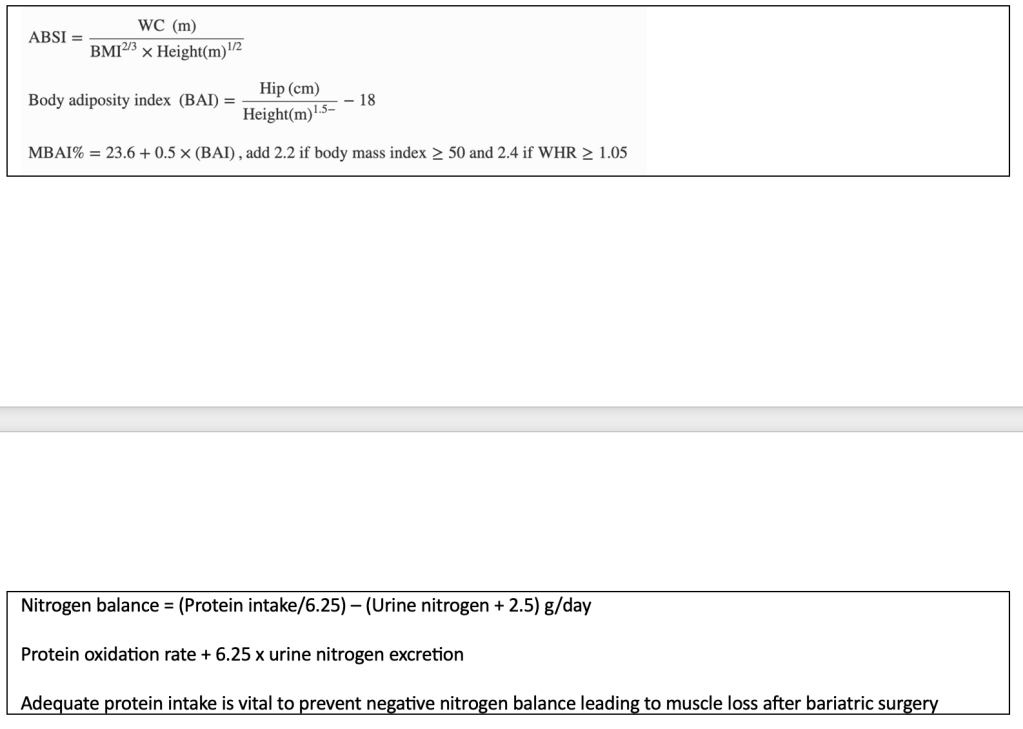
A body shape index (ABSI)
Modified body adiposity index (MBAI)
Definition of weight loss success
The ideal weight for everyone following the Caucasian standard is to have a BMI 20-25. The world’s population in the last few centuries rarely have morbid obesity issues.
This is obviously not the case any more in the 21st century.
With the introduction of bariatric surgery, there is also a need to define what constitutes successful weight loss surgery outcomes.
- Around 1982, surgeons began describing weight loss surgery as achieving >50% excess weight loss (EWL) and this has been the standard to which we measure the success of bariatric surgery ever since.
- More recently the definition of weight loss success after surgery include >20% (total body weight loss) TWL. This is easier to calculate and TWL getting used more often in modern day scientific research.
- Inadequate weight loss is defined as <50% EWL
In contrast the definition for success using medical pharmacology treatments (without bariatric surgery) is >5% TWL.
- However and fortunately reduction in medical co-morbidities can be seen after 5-10% TWL.
Some researchers have noted that:
- Weight loss surgery provides 4 times more weight loss in the long term
- Overall the successful long term weight loss (>20% TWL) is expected in 70% of patients
The definition of weight regain after bariatric surgery however is not clear at this stage.
There has been several suggestion, which include:
- BMI >35 after initial success of BMI <35 after the initial surgery
- EWL <50% after initial success of >50% EWL after the initial surgery
- Weight regain >25% EWL from the lowest weight (nadir)
- Weight regain >10-15% from the lowest weight (nadir)
- Not able to maintain >20% TWL at all
Less successful outcome (<20% TWL) is observed in:
- Gastric band surgery
- Higher pre-op BMI
- Patients with pre-op T2DM and HPT
- Age over 40 years
- Male gender
- Substance abuse (alcohol)
- Medical causes of weight regain
Weight loss results after bariatric surgery
Patients falls into 3 categories after bariatric surgery.
- Primary responder are patients who achieved >50% EWL.
- Primary non responder are patients who achieved <50% EWL (previously called failure of weight loss).
- Secondary non responder are primary responders with successful weight loss in the past but has regained the weight lost
- Mild regain is 5-10kg from the nadir
- Severe regain is >10kg from the nadir
Weight regain are often multifactorial and difficult to study.
In a simplistic explanation, they may be grouped as:
- Technical failure (eg. dilated proximal gastric pouch or loss of restriction and increased food portion size)
- Hormonal changes (eg, rise in ghrelin, loss of satiety)
- Nutritional non-compliance (eg. non adherence to dietician dietary plans, sweet eating)
- Behavioural non-compliance (eg. grazing, emotional eating habits)
- Inadequate physical activity
- Psychological factors
| Recent Modified Delphi consensus Expert opinion stating that: Suboptimal weight loss is <20% of total body weight loss within 2 years of surgery Recurrent weight gain is more than 30% of initial surgical weight loss |
| Resolution of T2DM after bariatric surgery It is also noted that bariatric surgery may halt the progression of T2DM, which is a chronic progressive disease, it is not necessarily about achieving a life-long cure. Secondly patients with relapse or persistence of T2DM were better managed and glycaemic control is easier after bariatric surgery. The restriction in calorie intake allows patients to reduce the medication doses for oral hypoglycaemics or insulin, as proven with better HbA1C blood tests results compare to patients who had medical treatment alone and did not have bariatric surgery. The success in treating T2DM often depends on other factors, such as: Advanced age of the patients Duration of the T2DM Whether patients are requiring or dependent on insulin In other words the ability of pancreatic Beta cells to recover, to regenerate/release insulin Patients are divided into 4 categories depending on their response after bariatric surgery. Complete remission of T2DM Originally defined as baseline blood glucose <100 mg/dL (5.6 mmol/L) and a HbA1C <6%, maintained for > 1 year without hypoglycaemic medications Newer definition is HbA1C <6.5% without medications Partial remission Defined as baseline blood glucose 100 – 125 mg/dL (5.6 – 6.9 mmol/L) or a HbA1C 6-6.5% without hypoglycaemic medications or those who have not discontinued hypoglycaemic medications Relapse Are patients who satisfied the criteria to define complete remission for more than 1 year but had recurrence of the diabetes, diagnosed as fasting glucose >126 mg/dL (7 mmol/L) or frank diabetes on oral glucose tolerance test >200 mg/dL (>11mmol/L) at 120 minutes Persistence Are patients who did not have characteristics necessary to define complete remission for a duration >1 year |
| Resolution of HPT and dyslipidaemia after bariatric/metabolic surgery Remission of HPT Blood pressure <135/85 without medication Remission of dyslipidaemia Triglyceride <150mg/dL and HDL >50 (females) or >40 (males) without medication |
| Definition of energy requirement Energy requirement (ER) calculation is based on the BMI BMI >35 ER = 35 kcal x adjusted body weight (BMI 22 or 25) BMI <35 ER = 35 kcal x body weight Malnutrition is defined as Moderate if patient consuming <3/4 of the hospital food tray and/or lost 5-15% of body weight Severe if patient consuming <1/2 of the hospital food tray and/or lost >15% of body weight |

